
Gallery



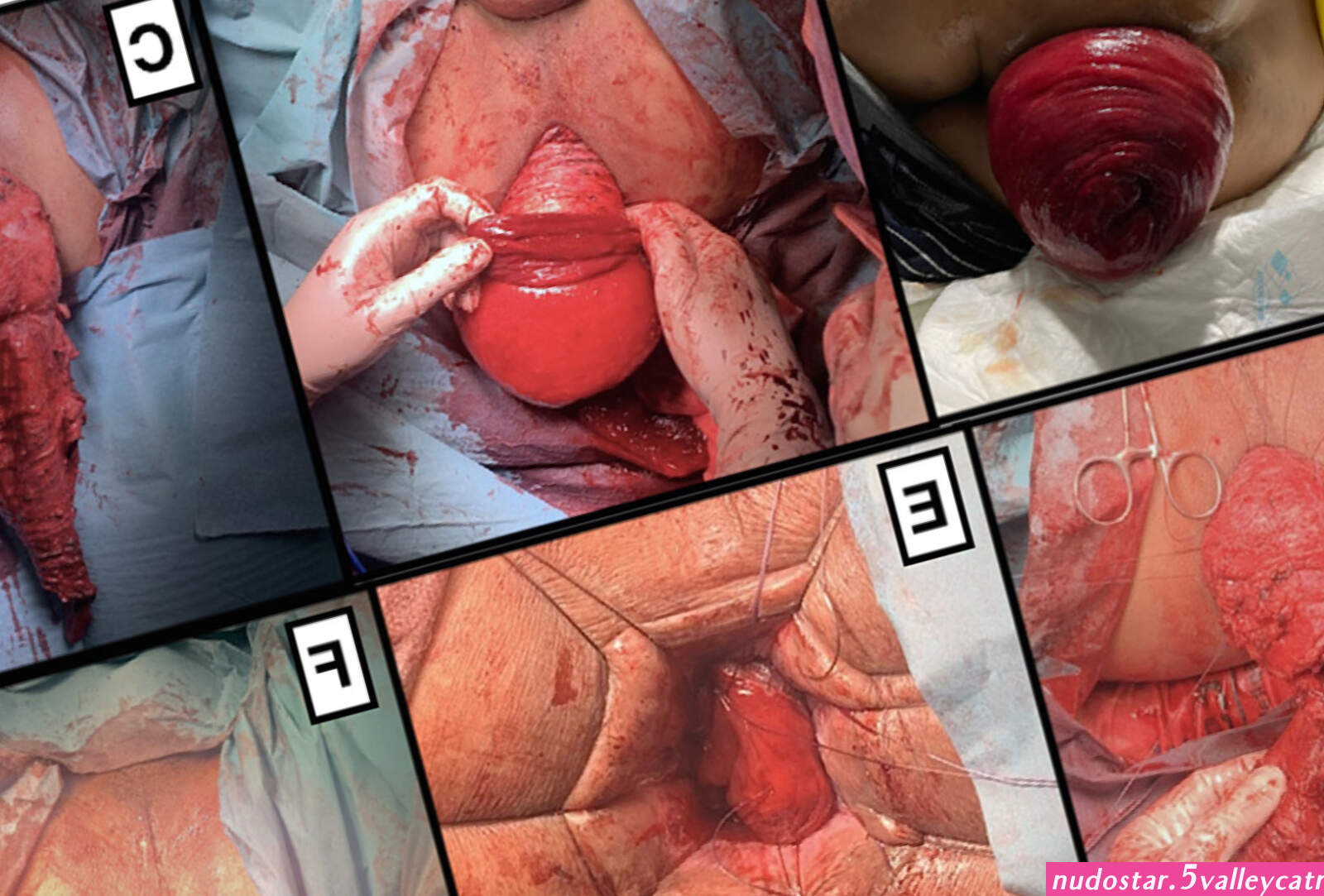




Rectal prolapse may be confused easily with prolapsing hemorrhoids. Mucosal prolapse also differs from prolapsing (3rd or 4th degree) hemorrhoids, where there is a segmental prolapse of the hemorrhoidal tissues at the 3, 7 and 11 o’clock positions. Mucosal prolapse can be differentiated from a full thickness external rectal prolapse (a complete rectal prolapse) by the orientation of the folds (furrows) in the prolapsed section. In full thickness rectal prolapse, these folds run circumferential. In mucosal prolapse, these folds are radially. The folds in mucosal prolapse are usually associated with internal hemorrhoids. Furthermore, in rectal prolapse, there is a sulcus present between the prolapsed bowel and the anal verge, whereas in hemorrhoidal disease there is no sulcus. Prolapsed, incarcerated hemorrhoids are extremely painful, whereas as long as a rectal prolapse is not strangulated, it gives little pain and is easy to reduce.
Sphincter function in rectal prolapse is almost always reduced. This may be the result of direct sphincter injury by chronic stretching of the prolapsing rectum. Alternatively, the intussuscepting rectum may lead to chronic stimulation of the rectoanal inhibitory reflex (RAIR – contraction of the external anal sphincter in response to stool in the rectum). The RAIR was shown to be absent or blunted. Squeeze (maximum voluntary contraction) pressures may be affected as well as the resting tone. This is most likely a denervation injury to the external anal sphincter.
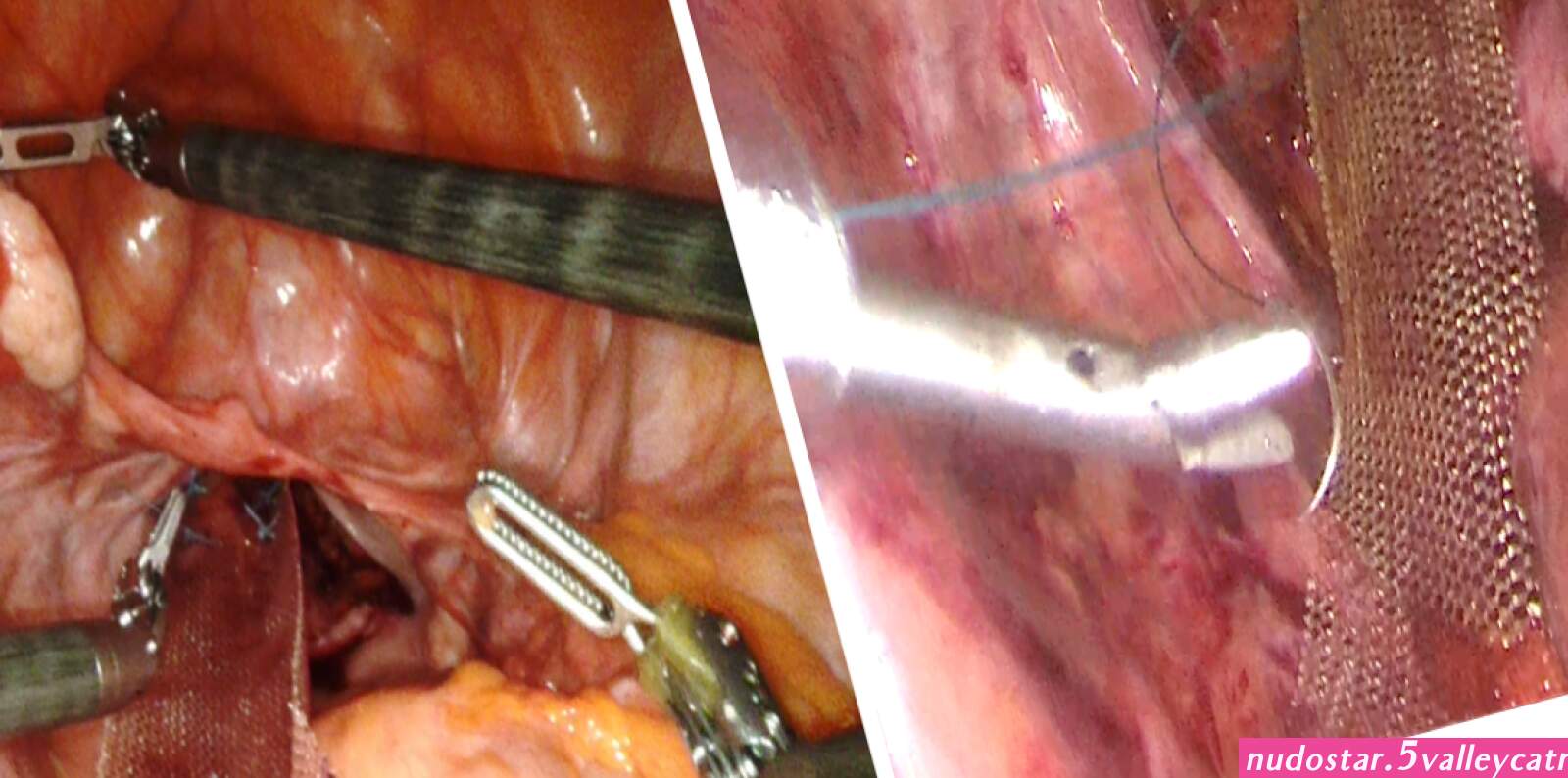
STATEMENT OF THE PROBLEM Rectal prolapse, internal intussusception, and solitary rectal ulcer syndrome comprise a spectrum of anatomical ab-normalities involving descent of full- or partial-thickness rectal wall associated with pelvic floor dysfunction. These conditions, although benign, can be extremely debilitating because of the discomfort of prolapsing tissue both internally and externally, associated drainage of mucus or blood, and the common occurrence of fecal incontinence or constipation. In patients with rectal prolapse, diastasis of the levator ani, an abnormally deep cul-de-sac, a redundant sigmoid colon, a patulous anal sphincter, and loss of the rectal sacral attachments are commonly found.1– 6 In times past, restoration of normal anatomy to treat rectal prolapse was considered a definition of success. However, the presence of multiple operations to correct this problem indicates that the achievement of excellent outcomes is somewhat elusive.
Related:
 Luvjazzxo onlyfans (photos)
Luvjazzxo onlyfans (photos)
 Ggg sexy susi (photos)
Ggg sexy susi (photos)
 Rena kodama creampie (photos)
Rena kodama creampie (photos)
 Camila elle fuck 974 (photos)
Camila elle fuck 974 (photos)
 Big boobs mom anal (photos)
Big boobs mom anal (photos)
 Woman get fucked (photos)
Woman get fucked (photos)
 Anal hd sexo (photos)
Anal hd sexo (photos)
 Big booty jamaican riding cock (photos)
Big booty jamaican riding cock (photos)
 Buen porno (photos)
Buen porno (photos)
 Stark behaart porno (photos)
Stark behaart porno (photos)
 Belinda bauer nude (photos)
Belinda bauer nude (photos)
 Lauren burch naked photos (photos)
Lauren burch naked photos (photos)
 Nudes lucy sofia (photos)
Nudes lucy sofia (photos)
 Mariewithdds (photos)
Mariewithdds (photos)
 Grace charis nude photos photos (photos)
Grace charis nude photos photos (photos)
 Mia sorety xxx leaked photos (photos)
Mia sorety xxx leaked photos (photos)

